Elective Surgery: Is Waiting in the Public System Worth It? Australia Wait Times, Medicare and Private Options Compared (2026 Update)
Public elective surgery can save you thousands, but the wait may be weeks, months or longer depending on your urgency category, procedure and state. Here’s how Medicare, public waitlists and private hospital options compare in Australia in 2026.


If you've been told you need surgery that isn't an emergency, you've probably been handed two options: go public and wait, or go private and pay. I had the same question when a family member was told they needed a knee procedure. The surgeon mentioned a public waiting list of several months, but also handed over a quote for private treatment that made us pause. What followed was a lot of reading and a few confusing phone calls before we felt like we understood what was actually on offer.
Like a lot of Australians, I assumed public meant free and straightforward. Then I started hearing about friends waiting 12 months for a hernia repair, and others who paid thousands to skip the queue. Today we'll break down how elective surgery wait times actually work in the public system, what Medicare covers, and when paying privately might make sense for your circumstances.
This is for Australian adults with a Medicare card who are weighing up public waitlists against private health insurance or paying out-of-pocket.
Short answer first
Elective surgery in Australia's public hospitals is available to all Medicare card holders and you won't pay for the surgeon or hospital stay if you're treated as a public patient, if you meet the rules. But "elective" doesn't mean optional — it means planned surgery that's medically necessary but not an emergency.
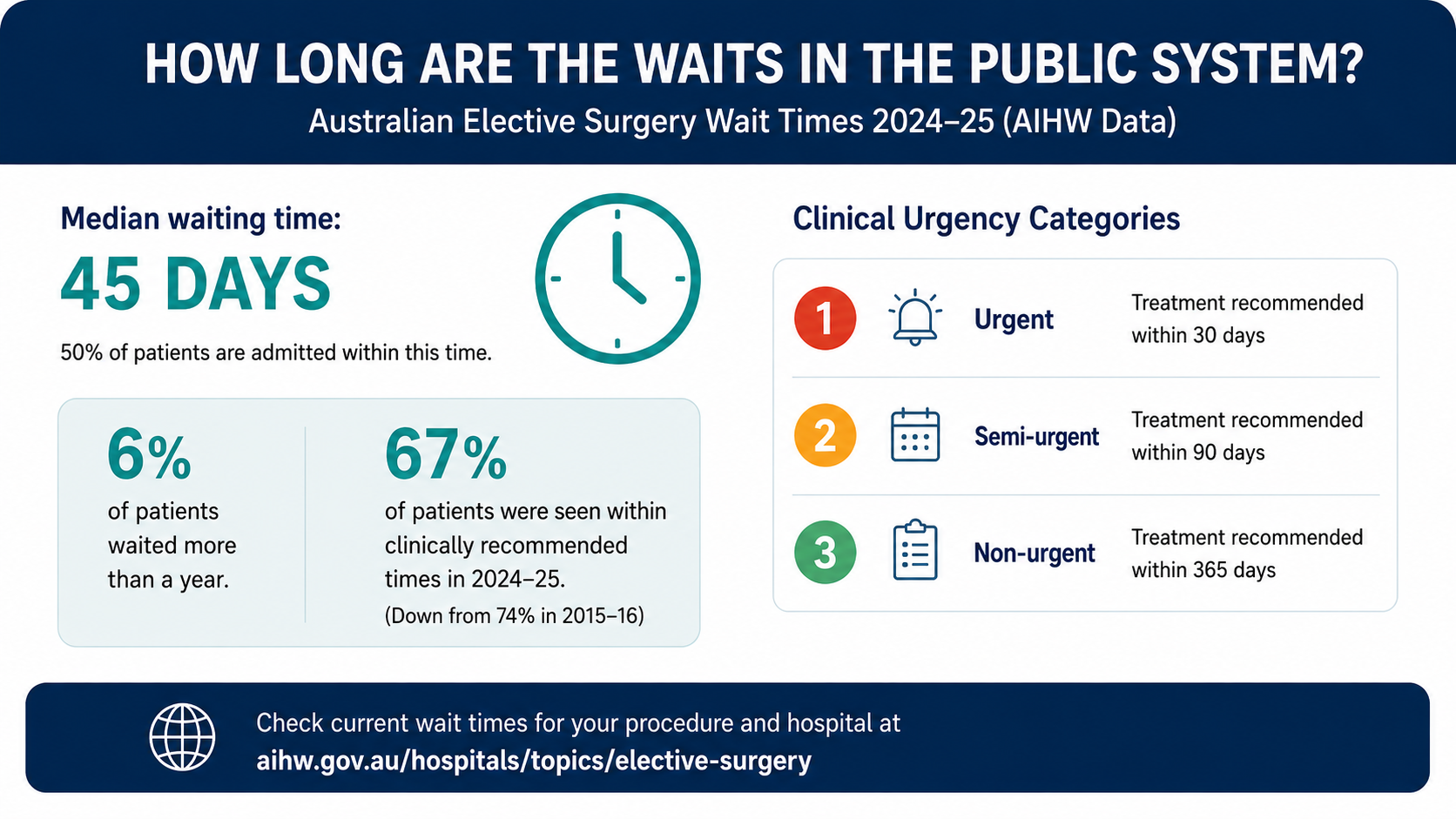
As of June 2026, AIHW elective surgery data for 2024–25 shows the median waiting time was 45 days, and 50% of patients were admitted within that time. But 6% waited more than a year, and it varies a lot by procedure, urgency category, and which state you're in.
Most private hospital cover will reduce wait times if your policy includes the treatment and you've served any waiting periods.
Whether waiting is worth it depends on your clinical category, how the condition affects your life, and what you can afford. Check current wait times on the AIHW elective surgery waiting times page, and check your own Medicare situation through Services Australia.
Elective surgery in plain English
Elective surgery sounds like it's optional, but in the health system it just means planned surgery that's medically necessary and not an emergency. Think cataract removal, hip or knee replacements, gallbladder removal, hernia repairs, and tonsillectomies.
Under Medicare, public patients in public hospitals don't get a bill for the surgery itself. Medicare and the state government cover the cost of your surgeon, anaesthetist, theatre and ward stay. You can read more about how Medicare works through Services Australia’s health care and Medicare page.
You're assessed by a specialist first, then placed on the waitlist as "ready for care" once you're medically fit for surgery.
In the public system, the usual pathway looks like this:
- you see a GP
- your GP refers you to a specialist or public hospital clinic
- a specialist assesses whether surgery is needed
- if surgery is recommended, paperwork is sent to the hospital
- you are placed on a public hospital waiting list
- the hospital schedules surgery based on urgency, capacity and clinical priority
Your spot in the queue comes down to three clinical urgency categories used nationally:
- Category 1 – urgent: treatment recommended within 30 days
- Category 2 – semi-urgent: treatment recommended within 90 days
- Category 3 – non-urgent: treatment recommended within 365 days
The surgeon decides the category based on clinical need, not on how long you've already waited or how uncomfortable you are, though worsening symptoms can lead to a review. Elective surgery waiting lists are not simply first come, first served — patients are prioritised by clinical urgency, which is why two people waiting for the same operation may not receive the same date.
Those timeframes are recommended clinical targets, not a personal guarantee. Your actual wait can depend on the procedure, hospital capacity, staffing, theatre availability and whether your condition changes while you wait.
The word "elective" is confusing
This trips a lot of people up. "Elective" doesn't mean cosmetic or low priority. A brain aneurysm repair can be Category 2 elective. A Category 1 procedure could still be serious surgery — it's just not done in the emergency department that day.
The other common confusion is between elective and cosmetic. Elective surgery in this context refers to medically necessary planned surgery. Purely cosmetic procedures are different and may not be covered by Medicare or private health insurance in the same way.
Another misunderstanding: "free" doesn't mean "fast." Public hospitals juggle emergency cases, staff availability and theatre time. Even urgent cases can be delayed if the system is under strain. As of the Productivity Commission’s Report on Government Services 2026, 67% of patients were seen within clinically recommended times in 2024–25, down from 74% in 2015–16.
Also worth knowing: when you see official waiting time figures, they're usually based on people who have already been admitted for surgery — not a live promise about how long you personally will wait.
If you're reading an article from 2021 quoting COVID backlog stats, double-check the date. Things shifted. The median wait peaked at 49 days in 2022–23 and has come back to 45 days in the latest 2024–25 data.
Urgency categories and where they matter
Your category is the single biggest factor in how long you wait. It's based on clinical need, not how long you've been waiting or how much pain you're in, though severe pain can influence the surgeon's decision.
Where people get caught out:
- Your category can change. If your condition deteriorates, go back to your GP or specialist. The hospital can only act on the latest referral.
- "Not ready for care" pauses the clock. If you postpone for a holiday, or you need to get fitter first, you won't be counted as overdue, but your total calendar time gets longer. If you postpone, tell the hospital. Otherwise you might be removed from the list entirely.
- It varies by state and procedure. Total knee replacement in 2023–24 had a median wait of 321 days in NSW, 181 days in Victoria, and 276 days in Queensland. In 2024–25, cataract extraction had a median wait of 106 days nationally, while septoplasty was 320 days. Check early before assuming the public timeline works for you.
- Symptoms changing while you wait. If your condition worsens, don't assume the hospital automatically knows. Contact your GP or specialist and ask whether your clinical information needs updating. A change in symptoms doesn't mean your surgery date will automatically move forward, but the treating team should have current information.
You can look up your procedure by state on the AIHW elective surgery waiting times page. If you want to see waiting times by patient characteristics, AIHW also has a separate page for waiting times by patient characteristics.
Who actually qualifies?
Any Medicare card holder can be placed on a public hospital elective surgery waitlist if a specialist says the procedure is clinically necessary. There's no income or assets test.
But eligibility is not just about the person; the hospital, timing and documents matter too. You'll need:
- a GP referral to a public hospital outpatient clinic
- assessment by the specialist who confirms surgery is needed
- to be medically fit and "ready for care" when a date comes up
If you're in NSW and want to understand the public pathway, NSW Health explains how patients join an elective surgery waitlist on its elective surgery waitlist page.
If you have private health insurance, you can still use the public system. Some people with Gold cover still go public for Category 1 surgery to avoid excess and gap fees. Others use their cover to pick their surgeon and date.
Hospital cover tiers determine what you're covered for. Gold covers all 38 clinical categories including joint replacements and pregnancy. Bronze and Basic often exclude joint replacements. Before assuming you're covered, check the hospital product tiers on PrivateHealth.gov.au and compare that with your own policy.
Private health insurance may fit in
Private hospital cover lets you be treated in a private hospital, or as a private patient in a public hospital. Services Australia explains how Medicare and private health insurance can work together on its private health insurance and Medicare page.
Things to watch:
- Waiting periods. Up to 12 months for pre-existing conditions, 12 months for pregnancy and birth, and 2 months generally. If you join only when you need surgery, you'll likely still wait.
- Restrictions vs exclusions. A "restricted" hip replacement means you're covered as a private patient in a public hospital, but only partly in a private hospital. "Excluded" means the insurer pays nothing for that service.
- Out-of-pocket costs. Even with cover, you may have an excess, and your surgeon or anaesthetist can charge above the MBS fee. One thing worth asking your insurer before you proceed: whether the surgeon you want participates in a no-gap or known-gap arrangement with your fund. If they do, your out-of-pocket exposure is either eliminated or capped. If they don't, you may be left with a gap that can be significant.
The Department of Health explains private health insurance out-of-pocket costs on its out-of-pocket costs page.
How the two pathways compare
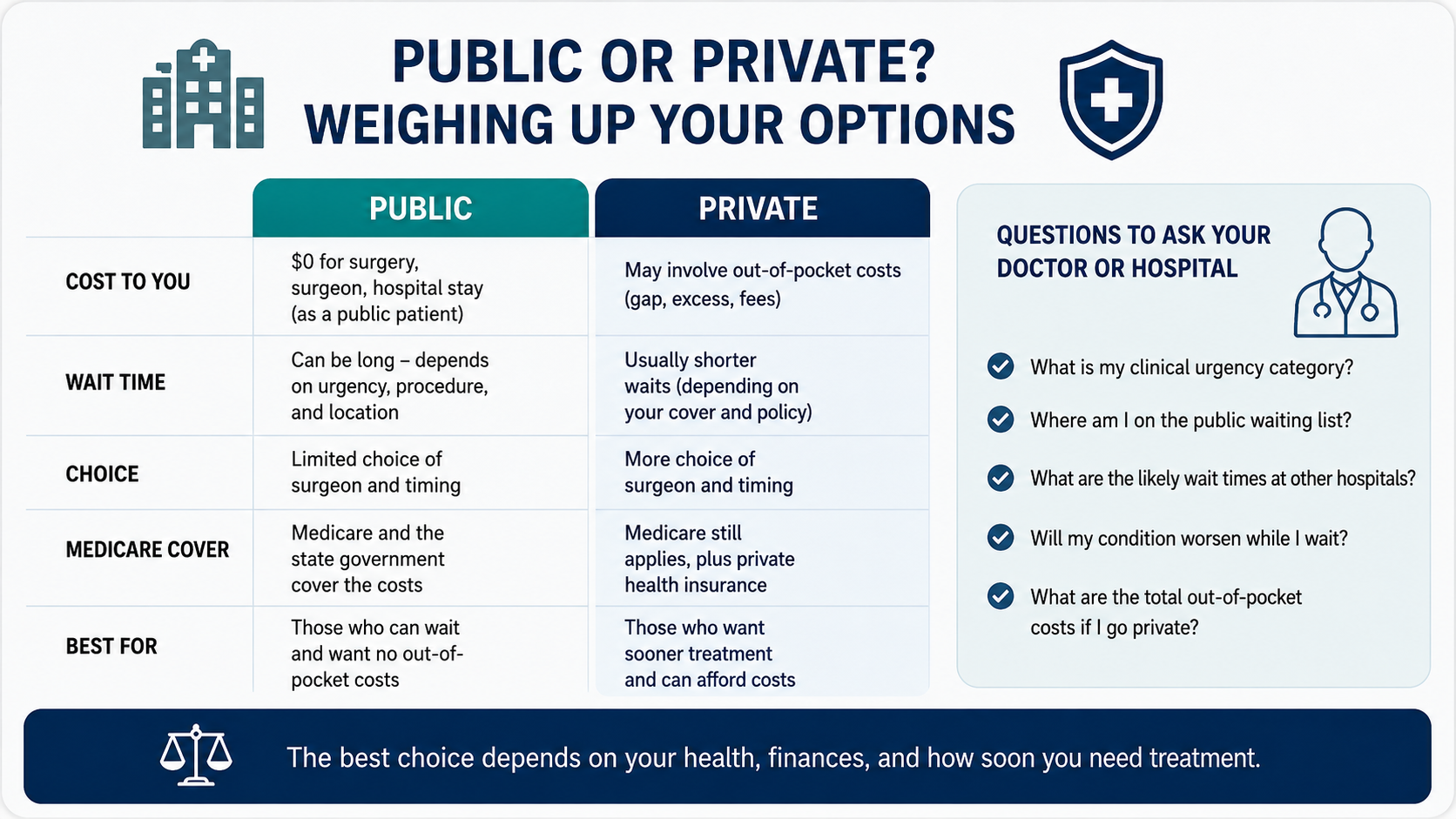
Public and private work differently. In public, you don't pay for the surgery itself, but you don't control the timing or who operates. As of June 2026, half of public patients got surgery within 45 days — but that's a median. Public patients specifically waited a median of 53 days, compared to 28 days for those using private health insurance for the same 25 most common procedures.
With private cover, you generally get a date within weeks and you choose your surgeon. But you'll have costs: your excess, plus any gap if the doctors charge above the MBS fee. Self-funding at a private hospital means no insurance waiting periods, but you pay the whole amount upfront — which for procedures like hip or knee replacement can be substantial.
Medicare covers 75% of the MBS fee for private in-hospital services; your insurer covers the other 25% if you're in an agreement hospital. But the surgeon's actual fee may be higher than the MBS fee, and that difference — the gap — comes out of your pocket unless they're in a no-gap scheme. You can search Medicare item numbers through MBS Online.
The trade-off is really time and choice versus cost. You can check typical costs by procedure and location using the Australian Government's Medical Costs Finder.
So when does this actually help?
If your Category 3 hernia isn't painful and doesn't limit work, the public wait may be fine. But if you're a tradie who can't lift for 9 months while waiting for a rotator cuff repair, the income loss might outweigh the private excess and gap combined.
This is most useful when you line up your category, local wait times and personal impact. You might have a Category 2 gallbladder issue with a 90-day recommended time, but your local hospital's median for that procedure is only 62 days — that could be manageable. But if it's a Category 3 knee replacement and your state median is 321 days, and you're in severe pain, private might be worth pricing out.
The public pathway can also be more suitable for complex medical situations. Public hospitals may have better facilities for complex conditions, emergency treatment or rural access. That doesn't mean private hospitals aren't appropriate — it means the best pathway depends on the condition and local services. Healthdirect has a plain-English overview of public and private hospitals in Australia, which can help if you're trying to understand the basic difference.
Private cover or self-funding tends to help when:
- You're Category 2 or 3, local waits are long, and the condition stops you working or sleeping
- You need certainty on timing for work or caring responsibilities
- You want a specific surgeon
Public works well when:
- You're Category 1 and will likely be seen within 30 days
- You can't afford premiums, excess, or gap fees, and the condition is manageable
- You're comfortable with the public hospital team and local waits are reasonable
State health departments publish dashboards. In Victoria, you can check the Victorian Agency for Health Information’s patients treated by urgency category page. In NSW, the NSW Health elective surgery waitlist page is a useful starting point.
Check those before you decide.
A few things to watch for
- Assuming elective means optional. Many elective surgeries are medically necessary. If symptoms change, pain worsens or function declines, ask your GP or specialist whether your status should be reviewed.
- Not asking about your urgency category. Hospitals may not be able to give an exact date early on, but you can ask which category you're in, whether the wait is likely to be weeks or months, and who to contact if your symptoms get worse.
- Assuming private means no cost. Even with Gold cover you may have an excess, a surgeon gap, anaesthetist fees, and assistant surgeon charges. These are separate bills that can add up to more than people expect. A surgeon's fee is only one part of the bill.
- Not confirming your insurance tier. Bronze doesn't cover joint replacements. Call your fund and ask specifically: "Is this procedure included, restricted or excluded?" If your policy is new or recently upgraded, ask whether waiting periods apply. You can compare hospital tiers through PrivateHealth.gov.au.
- Ignoring "not ready for care" status. If you postpone surgery, tell the hospital. Otherwise you may be removed from the list and need to start the whole process again.
- Not getting written cost estimates. You're entitled to an Informed Financial Consent document from your surgeon before any private procedure — a written breakdown of all expected costs including surgeon, anaesthetist and any assistant fees. Get this before agreeing to anything. The Australian Government's Medical Costs Finder can also help you understand typical costs before you ask for quotes.
- Forgetting the public option after buying insurance. You can still use Medicare services when you have private health insurance. In some cases, remaining a public patient may be the better option.
- Not checking the admission paperwork. If you want to be treated as a public patient, make sure the hospital paperwork reflects that. On your admission forms, look for "Election to be treated as a public patient".
How to check
Before deciding whether to wait publicly or explore private treatment, collect the details that actually affect your decision.
Start with your GP or specialist and ask:
- What procedure is being recommended?
- What urgency category am I in?
- What happens if I wait?
- What symptoms should make me seek review sooner?
- Are there non-surgical options worth trying first?
- Which hospital will the referral go to?
- Who should I contact if my condition changes?
If you're already on a public waiting list, contact the hospital booking office and ask:
- Am I on the waiting list?
- What date was I added?
- What procedure am I listed for?
- What urgency category am I in?
- What should I do if my symptoms get worse?
- Are my contact details up to date?
In your hospital letters, referral documents or patient portal, look for terms such as "elective surgery", "planned surgery", "waiting list", "Recommendation for Admission", "RFA", "urgency category", "ready for care", "pre-admission clinic" and "theatre booking".
If you're considering private treatment, ask your insurer:
- Is this procedure included under my hospital cover?
- Is it restricted or excluded?
- What excess applies?
- Is the hospital covered under an agreement?
- Will I have any waiting period?
- Does my surgeon participate in a no-gap or known-gap arrangement?
- Can I get a written estimate of what the insurer will pay?
Ask the surgeon's rooms for written details too. If your specialist gives you MBS item numbers, keep them — they help your insurer, surgeon's rooms and hospital give more accurate information. You can search item numbers through MBS Online.
Ask for Informed Financial Consent before agreeing to any private procedure. On hospital or insurer documents, search for words like "excess", "gap", "prosthesis", "restricted", "excluded", "waiting period" and "known gap".
For public patients, confirm you'll be admitted as a public patient so you don't accidentally get booked as private.
Official places to start:
- Services Australia – Medicare
- AIHW – Elective surgery
- AIHW – Elective surgery waiting times
- Medical Costs Finder
- PrivateHealth.gov.au – Hospital product tiers
The bottom line
Public elective surgery is free at point of care and works well for urgent cases, but wait times can stretch from weeks to over a year depending on your category, procedure and state — as of June 2026. Private hospital insurance or self-funding can reduce wait times and give you more choice, but comes with premiums, excesses and possible gap fees that need to be checked carefully before you commit.
The right path depends on your clinical urgency, financial position and how the condition is affecting your daily life. Neither option is universally better. The practical approach is to confirm your public waiting list status, understand your urgency category, ask what changes should trigger a review, and get written cost estimates before choosing private treatment.
Rules, waiting times and insurer agreements can change, so it is worth confirming directly with the hospital, specialist or insurer before making a decision based on your own situation.
Sources
- Australian Institute of Health and Welfare – Elective surgery
- Australian Institute of Health and Welfare – Elective surgery waiting times
- Australian Institute of Health and Welfare – Waiting times by patient characteristics
- Productivity Commission – Report on Government Services 2026, Part E Health
- Victorian Agency for Health Information – Patients treated by urgency category
- Services Australia – Health care and Medicare
- Services Australia – Private health insurance and Medicare
- PrivateHealth.gov.au – Hospital product tiers
- Department of Health – Medical Costs Finder
- Department of Health – Out-of-pocket costs
- Department of Health – Medicare Benefits Schedule
- NSW Health – How do I join an elective surgery waitlist?
- Healthdirect – Public and private hospitals: an overview
- CHOICE – Elective surgery: What you should know about public vs private hospitals